
Page 2 - Dyslipidaemia_newsletter8_2024_Final
P. 2
REFLECTIONS
Dyslipidaemia
Dyslipidaemia Global Newsletter #8 2024
For the first time, the new CCS guidelines describe an evolving that should be used and when they should be employed.
pathophysiological concept that highlights both functional and Dyslipidaemia
structural microcirculatory abnormalities as potential causes of Once a diagnosis is confirmed, the guidelines move on to
angina and ischaemia. They place greater emphasis on angina treatment strategies, covering a wide range of interventions,
and ischaemia in patients with non-obstructive coronary arteries including lifestyle modifications, drug therapy, and
by integrating for the first time INOCA and ANOCA endotypes. revascularisation procedures. The authors highlight the
importance of shared decision-making between patients and
The guidelines describe the clinical presentations of CCS, physicians, emphasizing the need for individualised treatment
emphasizing the diverse ways in which it can manifest, and then plans tailored to each patient’s specific needs and preferences.
delves into the diagnostic process. This involves estimating the The guidelines reinforce the importance of tailoring medical
likelihood of obstructive coronary artery disease (CAD) using therapy for symptom control in CCS according to each patient’s
a risk factor model, followed by non-invasive and invasive haemodynamic profile (e.g., HR, BP), comorbidities, and
testing to confirm the diagnosis. The guidelines provide detailed considering the specific pathophysiological mechanism of
recommendations for each step, specifying the types of tests myocardial ischaemia in each patient.
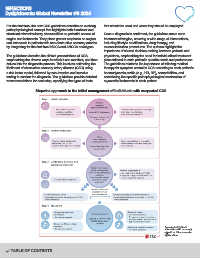
Stepwise approach to the initial management of individuals with suspected CCS
a In selected patients.
b Consider also coronary
spasm or microvascular
dysfunction.
TABLE OF CONTENTS